Machine Learning in Prognostic Decision-Support Systems Study - Computer Science Perspective
Details
Thank you for your interest in our study.
A primary role of doctors and clinicians is to assess the medical risk of patients exhibiting various symptoms and characteristics, and prescribe appropriate treatments and medical actions.
The purpose of the study is to investigate the factors that drive value for the use of Machine Learning models in generating prognostic predictions as part of decision-support systems for risk assessment designed to augment and complement the work of medical professionals and diagnosticians.
Many risk scores are currently embedded in electronic electronic health records; however these are based on logic rules and simpler statistical methods rather than Machine Learning algorithms, which can provide increased accuracy and other benefits, but may have perceived limitations in areas such as interpretability.
We are specifically looking to make Machine Learning algorithms more transparent, explainable, and interpretable by discovering how different model information and decision-support system design choices affect the confidence of medical experts in such systems.
The study proceeds in two stages:
About the model, which introduces and presents information regarding the Neural Network powering our Decision-Support System
Decision Support, which introduces a mock decision-support system designed to present predicted risk scores for patients
In this study, we focus on patients who have experienced heart failure, and predict the probability, or risk, of death one year after their heart failure event.
Please click below for full details before you start the survey.
General Information
Machine Learning, and more generally Artificial Intelligence, models are gaining enthusiasm for their ability to produce highly accurate predictive and analytical insights. However, as many such models, including neural networks, are black-boxes, many fields of practice are reluctant to utilise these models without an ability to interpret their results or understand how a model generates its prediction.
As a result, although ML models appear like natural and powerful choices for powering systems that support and augment decision-making processes for medical clinicians, there has so far not been a heavy push to incorporate these into practice in the medical field.
The aim of this study is to explore this phenomenon and understand what type of model evidence and interpretability modules will increase comprehension and the confidence levels for users in different machine learning predictive models utilised in decision-support systems for prognostics.
We appreciate your interest in participating in this online survey. You have been invited to participate as an expert in medicine, computer science, or related. Please read through these terms before beginning the survey. You will participate by ticking the Start box below. You may ask any questions before taking part by contacting the researcher (details below).
We, the University of Oxford, are investigating Machine Learning models in decision-support systems. You will be presented with a sequence of information on a machine learning model, followed by interactive patient scenarios and risk scores as may be presented by a decision-support system relying on the model described. You will then be asked to rate your confidence level with utilizing the system for decision-making purposes and support your answers.
The full survey should take about 15-20 minutes. No background knowledge is required. Your results will be utilised to determine the best interpretability modules and types of evidence to present to potential users of medical decision-support systems powered by machine learning models, and will be collected and utilised by the Computer Science and Engineering Departments at Oxford. No personally identifiable information will be collected or shared.
Do I have to take part?
Please note that your participation is voluntary. You may withdraw at any point during the questionnaire for any reason, before submitting your answers, by closing the browser. None of your answers will then be collected.
How will your data be used?
Your answers will be completely anonymous, and we will use all reasonable endeavours to keep them confidential. No personally identifiable information, including but not limited to IP address, email address, or name, will be requested or collected.
Your answers will be stored in a password-protected file and may be used in academic publications. Your IP address will not be stored. Research data will be stored for a minimum of three years after publication or public release.
Who will have access to your data?
The University of Oxford is the data controller for the purposes of the Data Protection Act 1998.
We would like your permission to use your unidentifiable data in future studies, and to share data with other researchers (e.g. in online databases).
Any personal information that could identify you will not be collected or be removed before files are shared with other researchers or results are made public.
This survey is for an MSc project. The principal researcher is Owen Lahav, who is attached to the Department of Computer Science at the University of Oxford. This project is being completed under the supervision of Mihaela van der Schaar of the Oxford Man Institute. This project has been reviewed by the University of Oxford’s Department of Computer Science’s Research Ethics Committee.
What if there is a problem?
If you have a concern about any aspect of this project, please speak to the researcher at oren.lahav@gtc.ox.ac.uk who will do his best to answer your query. The researcher should acknowledge your concern within 10 working days and give you an indication of how they intend to deal with it.
If you are over 18 and have read the information above and agree to participate with the understanding that the data (including any personal data) you submit will be processed accordingly, please click the ‘Start’ box below to get started. By doing so you will be providing your consent to participate.
Instructions:
Please carefully review the information presented and answer the questions on the screen.
Please do not use the back/forward or refresh buttons once you have started the survey.
Start
This version of the survey is designed for those with background in Machine Learning or computer science.
If you are ready to begin, please press start:
Part 1: About the Model
Starting on the next screen, you will be presented with information and evidence about the Machine Learning Model that was used to create a decision-support system to present to medical experts.
Please review each piece of information about the model and indicate your personal belief regarding whether doctors would find this information useful in increasing their comprehension of, and confidence in, the ML model and decision-support system based on it.
Click 'Next' to proceed
Part 1: About the Model
Please consider the following:
Data
The model was trained using the Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) data-set, which compiled patient data from 30 studies including both randomized clinical trials and observational registries.
The data set included 30,389 patients who have experienced a heart failure event. Of these, 18.8% died within 1 year of experiencing heart failure.
Note that all risk scores reported are for patients who have already experienced heart failure.
Of the 30,389 patients, 66% were male. The average age was 68, with a standard deviation of 12 years.
31 patient characteristics, symptoms, and other features were collected, including:
Basic patient details: Age, gender, ethnicity
Patient habits: BMI, Smoking, Diabetes condition
Physical symptoms: Shortness of breath (at rest and exercise), rales
Data and test results: Systolic and diastolic blood pressure, ejection fraction, etc.
New York Heart Association Score (Class I-IV) - click here for details
Missing values were imputed using standard methods (Multiple Imputation by Chained Equations), which provide accurate estimates for missing or not-recorded patient symptoms and characteristics
More details about the MAGGIC data-set, including a full list of features, can be found in (Pocock et al., 2012).
How useful do you believe medical experts would find this information about the data used to train the model powering a decision-support system for heart failure patients?
1: Not useful - Doctors will likely not understand or care about this information, and it will not impact their opinion of the model or decision-support system
2: Somewhat useful - This information will likely contribute to doctors' understanding and makes them somewhat more confident in the model and decision-support system
3: Very useful - This information will improves doctors' understanding and make them significantly more confident in the model and decision-support system
Please provide any comments or reasons supporting your answer:
Model Training and Implementation
The model utilised was a Neural Network, a sophisticated deep learning algorithm that has seen increased attention in recent years, as multiple studies have shown it to vastly outperform simpler linear models and other methods that have been traditionally utilised to generate risk scores in medicine.
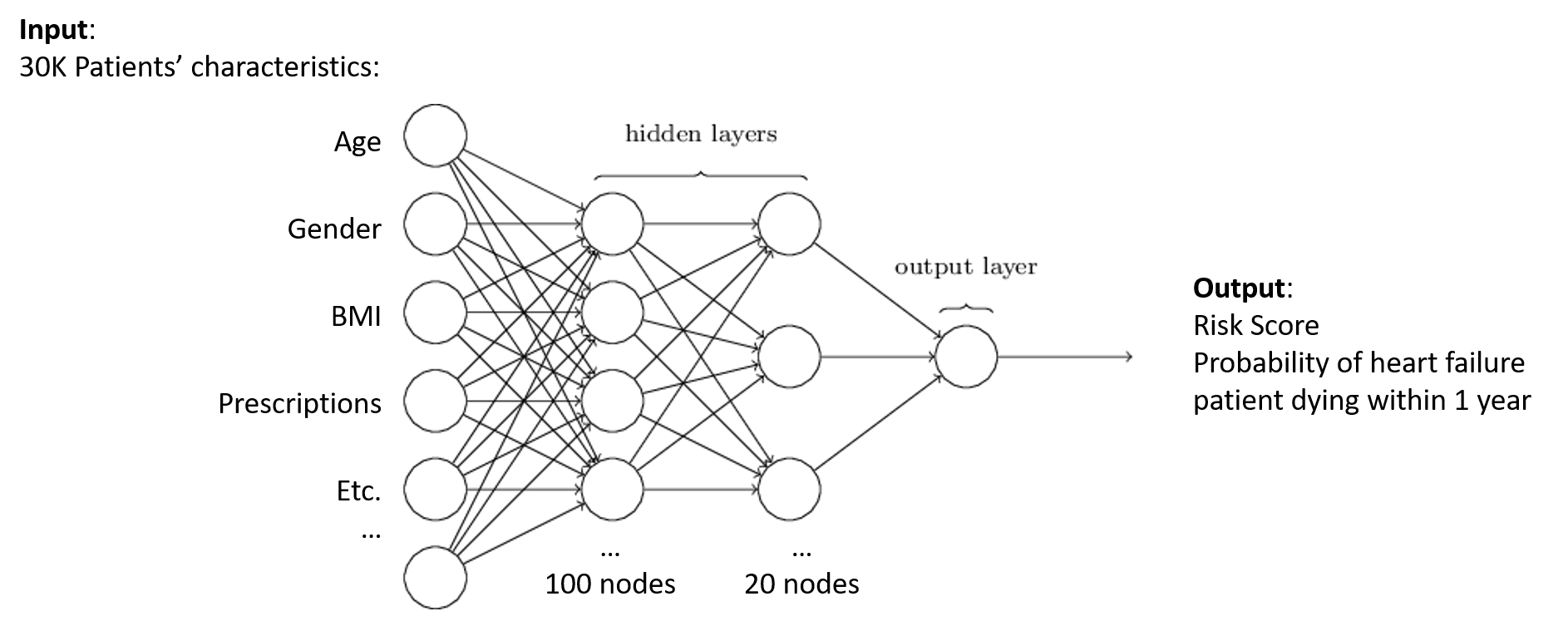
A neural network is a Machine Learning algorithm inspired by the human brain, utilizing connected nodes organised in hidden layers. With a single node and layer, the network would be essentially equivalent to a the linear predictive model known as Logistic Regression. However, adding nodes and layers enables the network to learn more complex, non-linear patterns in the data.
The network uses optimization techniques and non-linear activation functions to automatically discover these complex patterns and learn how to make predictions from data. You can find more information here.
Below is a generic image of a neural network by Machine Learning expert Michael Nielsen:
The network takes in a large amount of data, in the form of patient characteristics or features, and outputs the probability of a patient dying within 1 year of a heart failure event.
The Neural Network we utilised contained 2 hidden layers of 100 and 20 nodes respectively. In general, as explained here, network architecture, including the number of nodes and layers, must be tweaked and tuned to ensure the network is large enough to capture complex data patterns, but not too large compared to the size of the data-set, which would result in over-fitting and poor predictive performance in practice. The architecture we have selected of 2 layers with 100 and 20 nodes, respectively, was tuned and found to achieve highly accurate results.
The model was trained using 10-fold cross validation, using 90% of the data for training and the rest for testing. This was repeated 10 times, and we report average figures over the run. For more information on cross-validation, click here.
How useful do you believe medical experts would find this information about the architecture and training methodology behind the model powering a decision-support system for heart failure patients?
1: Not useful - Doctors will likely not understand or care about this information, and it will not impact their opinion of the model or decision-support system
2: Somewhat useful - This information will likely contribute to doctors' understanding and makes them somewhat more confident in the model and decision-support system
3: Very useful - This information will improves doctors' understanding and make them significantly more confident in the model and decision-support system
Please provide any comments or reasons supporting your answer:
Model Accuracy
The neural network showcases 81.26% accuracy, which means that 81% of the test cases were classified correctly by the model.
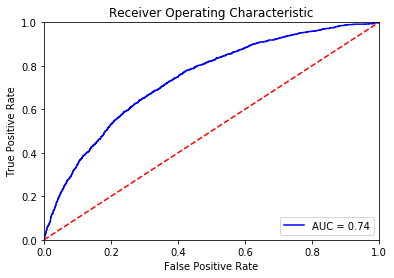
The model's AUC-ROC (area under the receiver operating curve), which is equal to the C-Index, is 0.725, with a standard deviation of 0.0054, averaged over 10 runs. This suggests high accuracy for the type of data, as we demonstrate below by comparing our network to a simple linear model and a risk score currently in use. For more information on the C-Statistic or AUC-ROC, click here.
The model's ROC curve is below:
In addition, the model achieves an AUC-PR (area under the precision recall curve) of 0.376. For more information about precision and recall, click here.
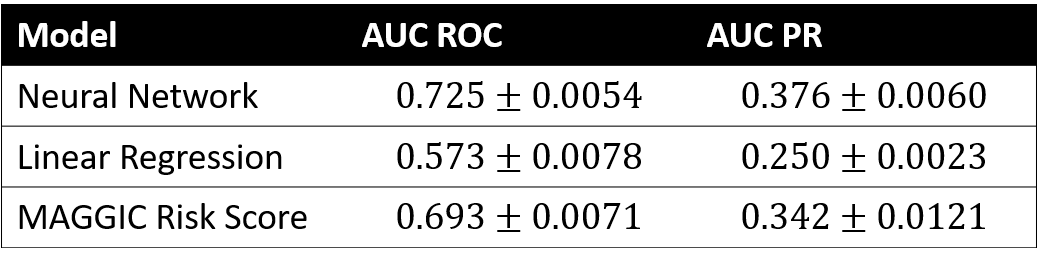
The neural network's accuracy values for both AUC-ROC and AUC-PR are much higher than the best linear regression model trained on the same data. They are also significantly higher than the accuracy of the MAGGIC Risk Score, an accepted risk score trained on the same data and developed by the European Society of Cardiology and other researchers. For information on the MAGGIC Risk Score, click here. The chart below summarises these results:
How useful do you believe medical experts would find this information about the accuracy of the model powering a decision-support system for heart failure patients?
1: Not useful - Doctors will likely not understand or care about this information, and it will not impact their opinion of the model or decision-support system
2: Somewhat useful - This information will likely contribute to doctors' understanding and makes them somewhat more confident in the model and decision-support system
3: Very useful - This information will improves doctors' understanding and make them significantly more confident in the model and decision-support system
Please provide any comments or reasons supporting your answer:
Model Interpretation: Stratified Linear Approximation
We have trained a neural network to predict the risk, or probability that a given patient who has suffered heart failure will die within one year of the heart failure event.
The model was trained on the data-set discussed previously, containing over 30K patients and 31 patient characteristics and features ranging from age to their New York Heart Association Score.
As shown previously, the neural-network outperforms simple linear models. However, the network is a black-box, which means it is impossible to tell how patient characteristics contribute to the outputted risk scores it produces.
In order to better understand how the model produces a prediction, black-box models, like neural networks, can be approximated locally using simpler models, including linear regression models.
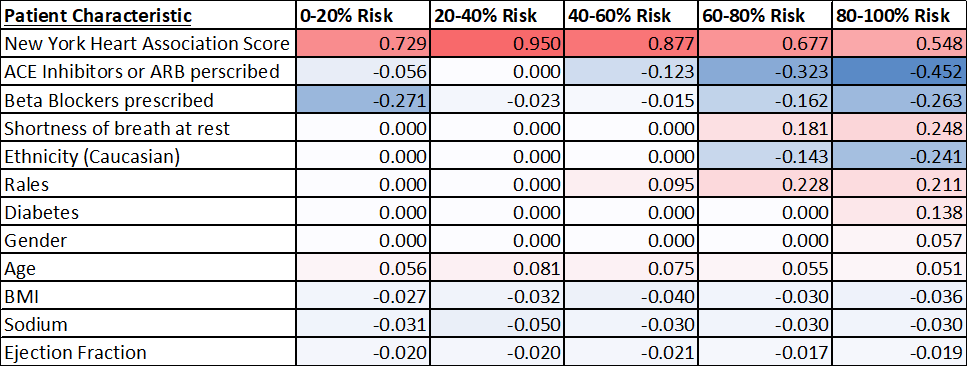
To create local approximations, after the neural network generated its risk scores, a different linear model was trained for each quintile of risk: 0-20%, 20-40%, etc.
The Root Mean-Squared Error between the neural network model and the linear approximation is 0.036, suggesting the 2 models are very close.
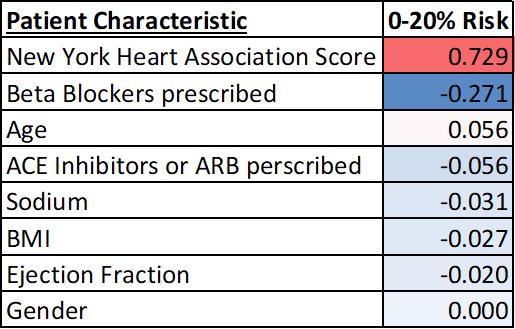
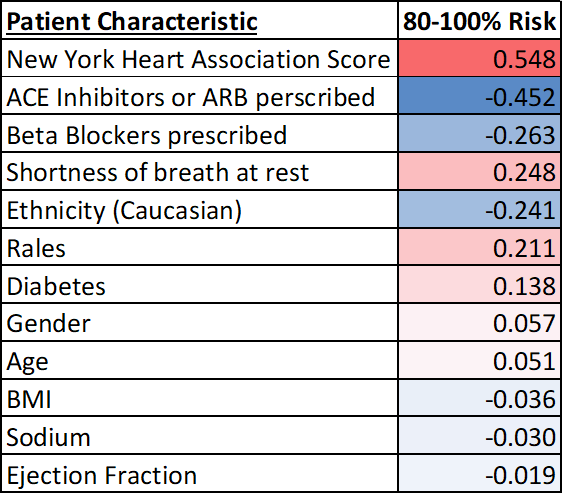
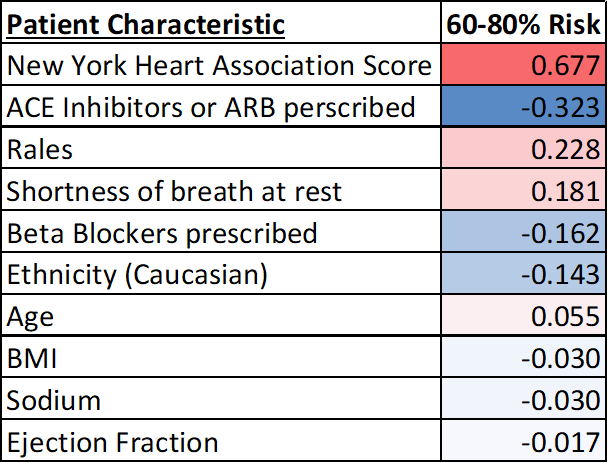
Below is a summary of the coefficients for each local linear model:
Since the linear approximation and the neural network models are so close, the value of each characteristic’s coefficient closely approximates their contribution to the variability in predicted patient risk score.
For instance, the negative coefficient for Beta blocker prescriptions suggests a negative correlation between this variable and risk of death, though the magnitude differs among risk strata. Some factors, such as shortness of breath at rest or gender, are only significant for high risk groups.
How useful do you believe medical experts would find this local linear approximation of the model powering a decision-support system for heart failure patients?
1: Not useful - Doctors will likely not understand or care about this information, and it will not impact their opinion of the model or decision-support system
2: Somewhat useful - This information will likely contribute to doctors' understanding and makes them somewhat more confident in the model and decision-support system
3: Very useful - This information will improves doctors' understanding and make them significantly more confident in the model and decision-support system
Please provide any comments or reasons supporting your answer:
Model Interpretation: Decision Tree
We have trained a neural network to predict the risk, or probability that a given patient who has suffered heart failure will die within one year of the heart failure event.
The model was trained on the data-set discussed previously, containing over 30K patients and 31 patient characteristics and features ranging from age to their New York Heart Association Score.
As shown previously, the neural-network outperforms simple linear models. However, the network is a black-box, which means it is impossible to tell how patient characteristics contribute to the outputted risk scores it produces.
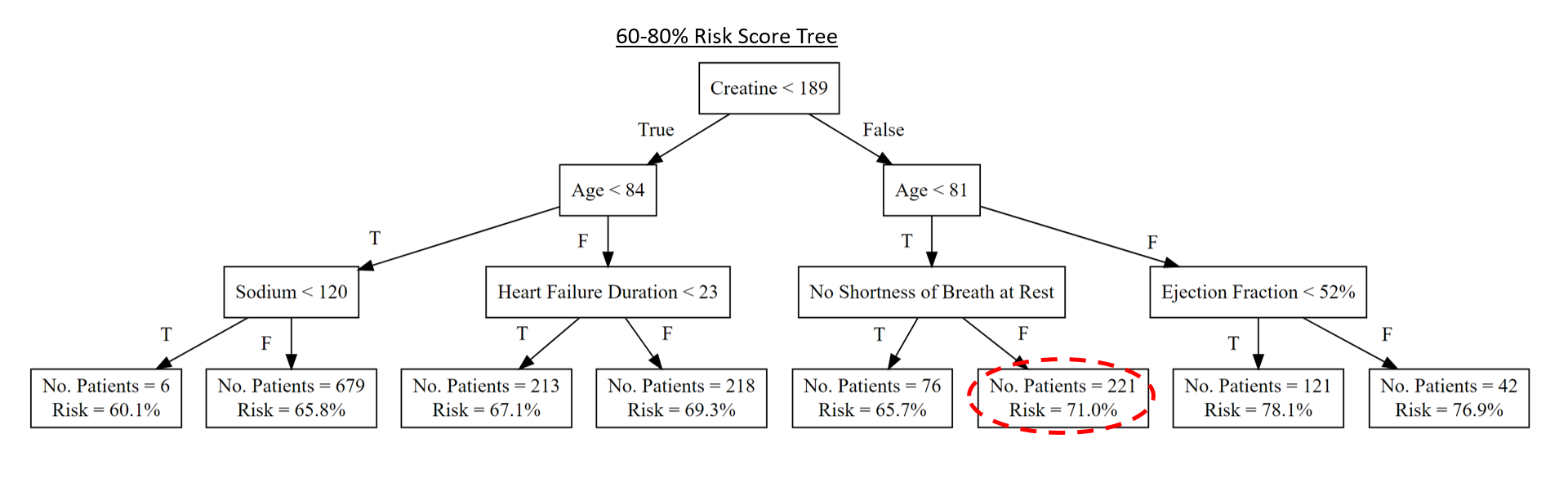
In order to better understand how the model produces a prediction, black-box models, like neural networks, can be approximated using simpler models, such as decision trees.
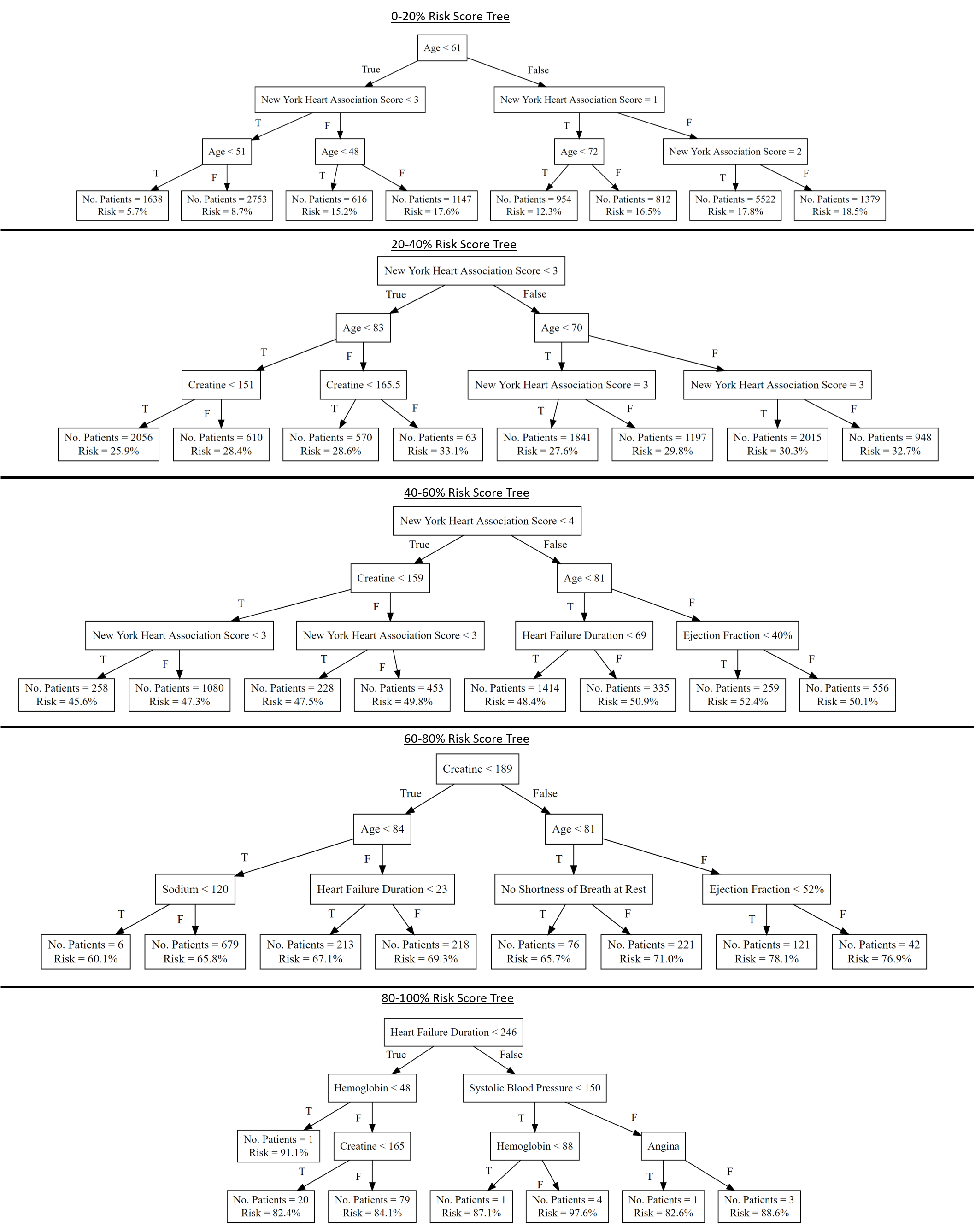
To create local approximations, after the neural network generated its risk scores, a different decision tree was trained for each quintile of risk: 0-20%, 20-40%, etc.
The Root Mean-Squared Error between the neural network model and the decision tree approximation is 0.046, suggesting the 2 models are very close.
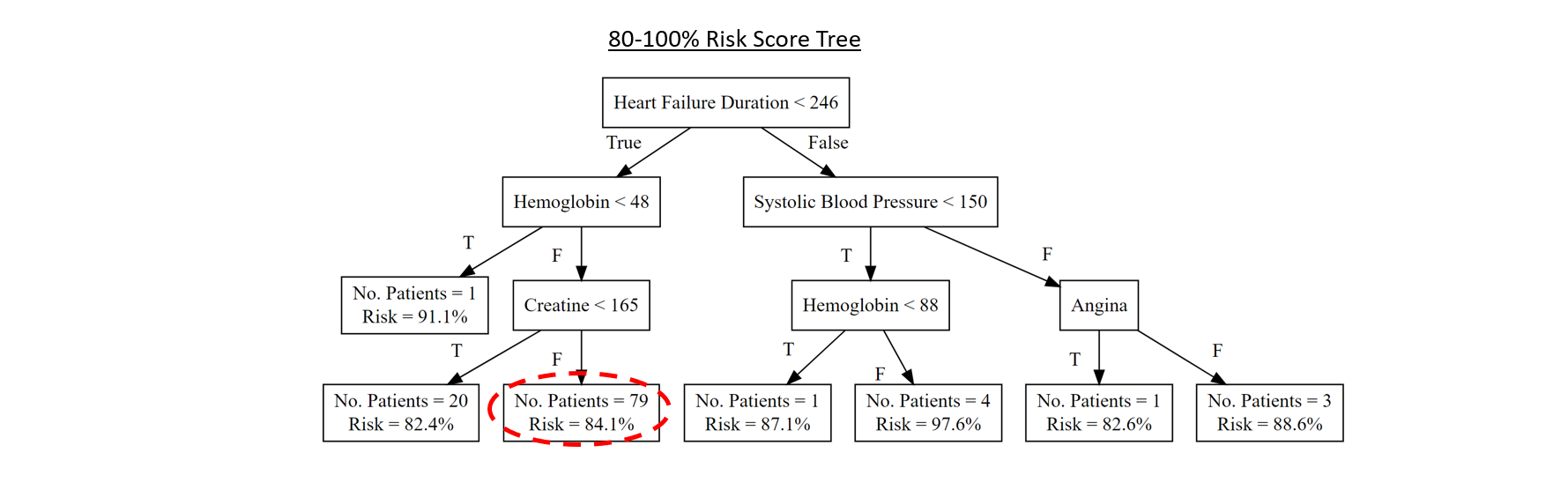
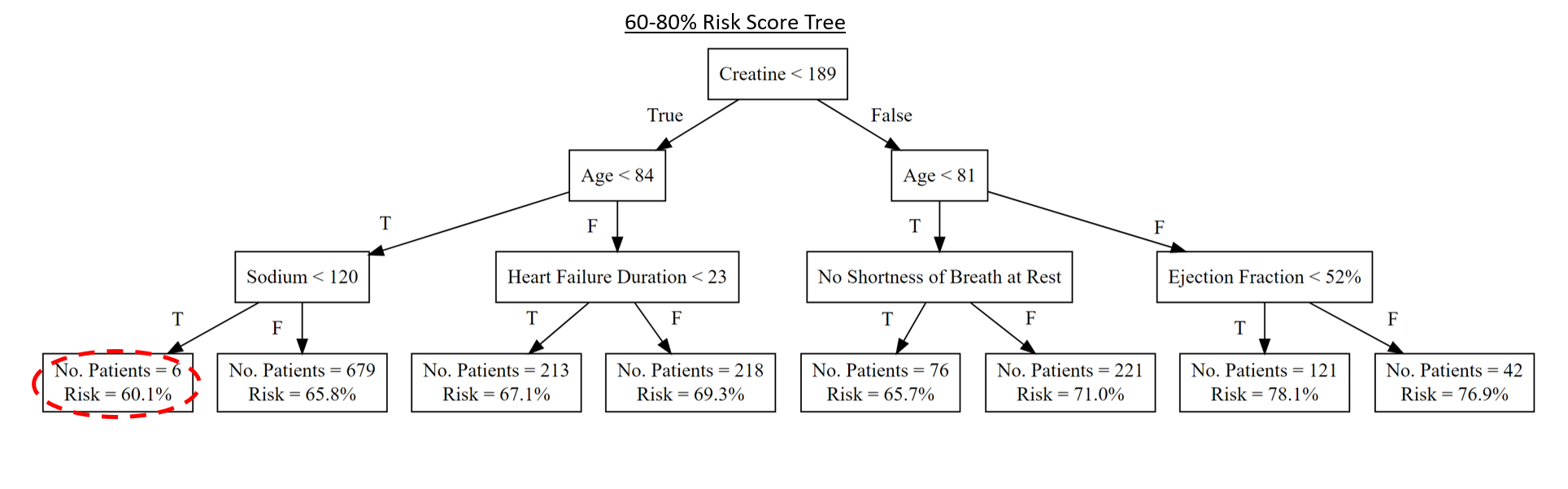
Click below for a summary of the depth-3 trees for each local linear model:
Note that each risk stratum utilises different patient characteristics for classification. Few patients are classified in the 80-100% class.
Since the models are so close, we can view the trees as an approximation explaining how each patient is assigned a risk score based on their characteristics and symptoms.
How useful do you believe medical experts would find this decision-tree approximation of the model powering a decision-support system for heart failure patients?
1: Not useful - Doctors will likely not understand or care about this information, and it will not impact their opinion of the model or decision-support system
2: Somewhat useful - This information will likely contribute to doctors' understanding and makes them somewhat more confident in the model and decision-support system
3: Very useful - This information will improves doctors' understanding and make them significantly more confident in the model and decision-support system
Please provide any comments or reasons supporting your answer:
Rate your confidence
Please consider the following question based on all the Model information and evidence seen so far:
Suppose the evidence seen so far was presented to an series of clinicians, doctors, and medical experts. On average, how would you expect doctors to rate their confidence in the machine learning model and the decision-support system based on it?
1: Not at all confident, would not even consider looking at the model and its prediction as part of their decision-making process
2: Not very confident, unlikely to consider model
3: Somewhat confident, doctors may consult model but unlikely to rely on it in any way
4: Fairly confident, likely to consult model and consider its predicted score
5: Very confident, almost certain to consult model together with other tools when considering further medical decisions
Please explain why you have selected the answer above, providing more detail about:
How the model details and evidence shown might affect doctors' confidence in a decision-support system
Which information would be most and least effective
What else you would have liked to see
Part 2: Decision Support System Providing Risk Assessment
We next focus on a Decision Support System providing Risk Assessment. Such a system is designed to support the decision-making processes of doctors facing patients exhibiting certain characteristics, symptoms, and conditions.
The system supports decisions on relevant medical actions by providing a predicted risk score, as well as background and explanations of the score. The system does not make treatment recommendations. However, the information provided may assist treatment decisions by explaining how different patient risk factors may contribute to predicted outcomes.
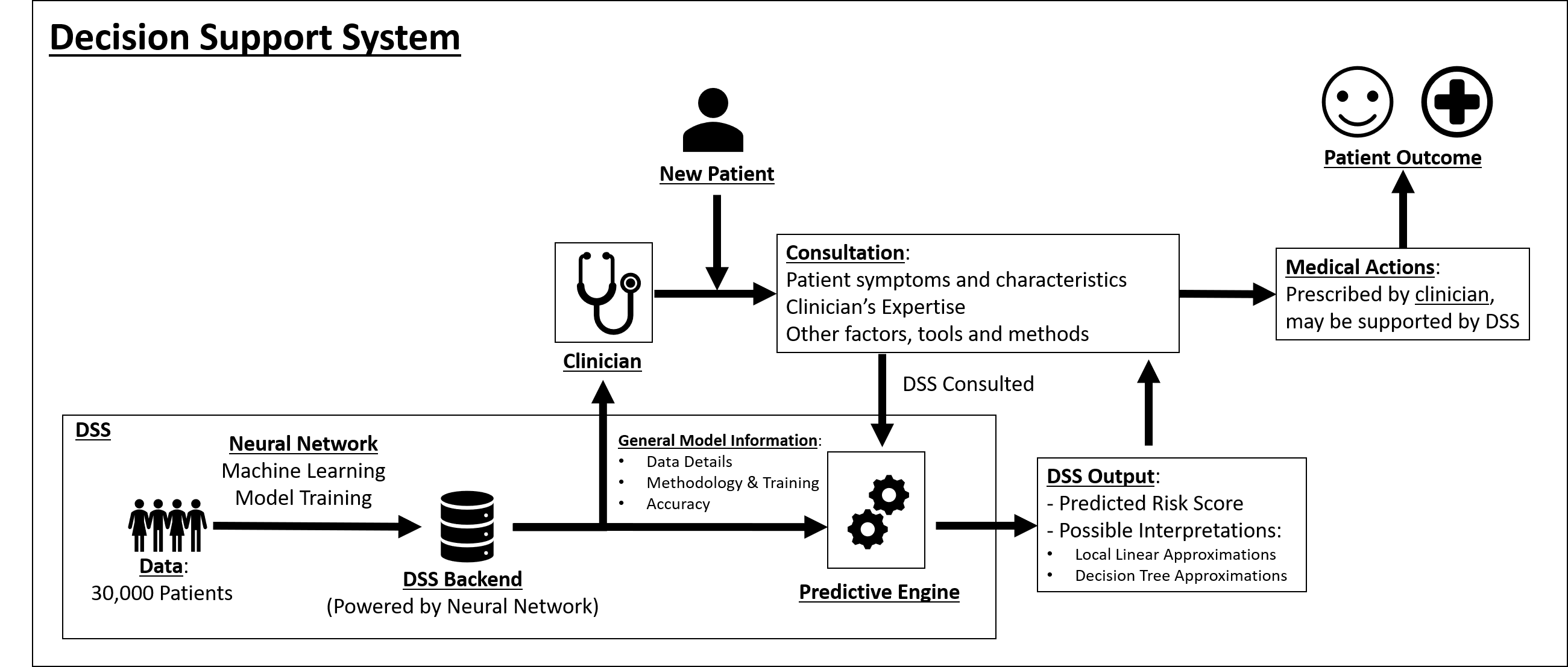
The following diagram explains the purpose and workings of a Decision Support System (DSS) powered by the Neural Network method described in Part 1:
Note that the DSS is based on the Neural Network trained on data of over 30,000 patients. As new patients consult with their doctors, the clinician may refer to the decision-support system. The DSS will produce a predicted risk score based on the patient's characteristics, and may additionally output relevant local, high-interpretable linear or decision-tree models. The information produced may be utilised by a clinician to inform medical actions and impact patient outcomes.
Starting on the next screen, you will be presented with a series of patients as part of a mock decision-support system.
Note that these patients were not part of the model's training set, and have been selected at random.
Each patient will be accompanied by a risk score generated using the Neural Network model discussed previously. In addition, medical information about the individual patients will be presented as well.
Please evaluate this information, and rate your expectation of the average doctor's satisfaction with the model and the decision-support system as a whole.
Click 'Next' to proceed
Part 2: Decision Support System Providing Risk Assessment
The following represents a patient scenario. A Decision Support System outputs a risk score based on the patient's characteristics. A doctor may choose to use the information below, including the risk score, to inform their medical decisions.
Please examine the following patient:
Patient Adam, a 43-year-old Caucasian male, experienced heart failure.
Our model predicts that the probability of Adam dying in the one year following the event is 15.9%.
Adam has a BMI of 26.5, and exhibits rales and shortness of breath at exercise.
Adam has marked limitation of physical activity (New York Heart Association Score Class III).
Adam has not been prescribed either ACE inhibitors or Beta blockers.
Adam admits to being an occasional smoker. He does not suffer from diabetes.
Click below to interact with the system
Examine how the following factors might impact Adam's predicted risk score, based on the Neural Network model utilized:
Note: This is a demo only. A full decision-support system will include other patient characteristics. 2 randomly chosen characteristics that impact the risk score were included here. This interactive tool is not meant to propose medical actions. Its goal is to enable exploring of how different patient characteristics may impact their risk score.
Predicted Risk Score:
15.9%
12.9%
13.4%
15.1%
12.2%
12.6%
Click below to view the details of a linear approximation model for Adam's Risk Strata of 0-20%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear regression models.
A different model is trained for each risk quintile, 0-20%, 20-40%, etc.
Below are the coefficients for all significant characteristics of Adam's local linear approximation model. Note that the magnitude of the coefficients signifies how much the patient characteristic contributes to the risk score.
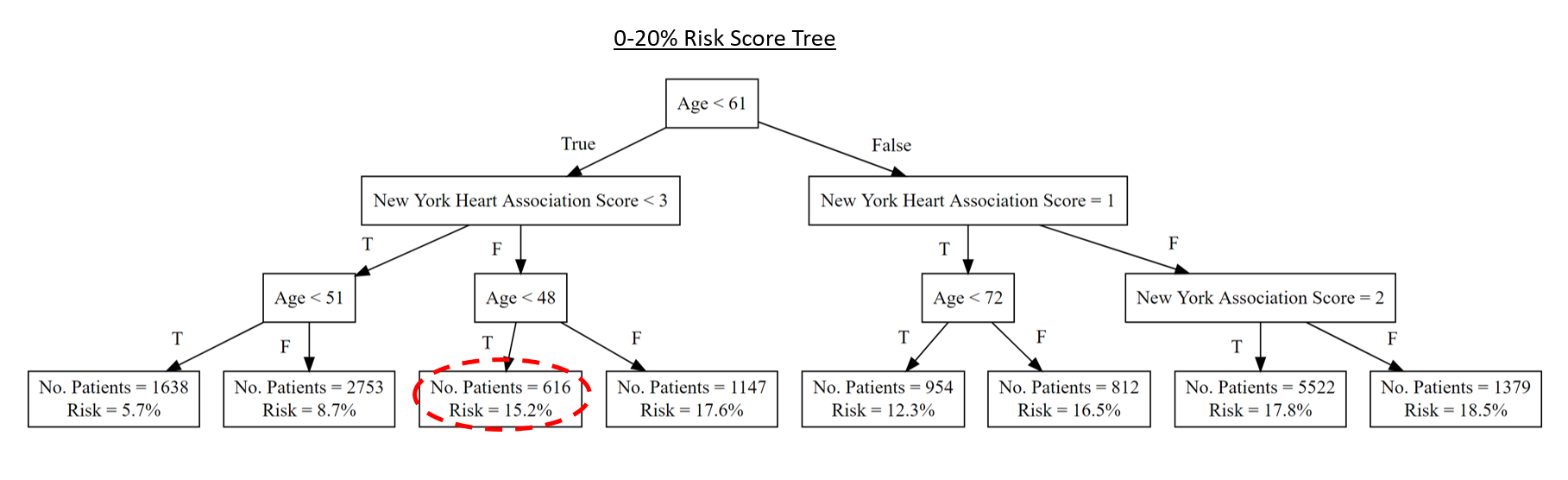
Click below to view the details of a decision tree approximation model for Adam's Risk Strata of 0-20%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear decision tree models.
A different tree is trained for each risk quintile, 0-20%, 20-40%, etc.
Below is a representation of Adam's local depth-3 decision tree approximation.
Click below to find the patient's status 1 year after the heart failure event
Patient Adam did not die in the year following diagnosis and in fact has survived for 7 years past his initial heart failure event.
Based on the information seen so far, including Patient Adam, how satisfied would you expect an average doctor to be with the Decision Support System powered by a Neural Network model?
1: Completely unsatisfied, not at all likely to use the system in supporting their medical decision-making for heart failure patients
2: Fairly unsatisfied, not likely to use the system
3: Neither satisfied nor unsatisfied, may or may not consult system
4: Somewhat satisfied, likely to at least take a look at the system's predicted risk score
5: Highly satisfied, very likely to consult the system and its prediction as part of their medical decision-making for heart failure patients
Please provide any comments or reasons supporting your answer:
The following represents a patient scenario. A Decision Support System outputs a risk score based on the patient's characteristics. A doctor may choose to use the information below, including the risk score, to inform their medical decisions.
Our model predicts that the probability of Betty dying in the one year following the event is 83.5%.
Betty has a BMI of 21.6, and exhibits rales and shortness of breath at rest.
Betty is unable to perform physical activity without discomfort (New York Heart Association Score Class IV).
Betty has not been prescribed either ACE inhibitors or Beta blockers.
Betty does not smoke, and does not suffer from diabetes. She does suffer from angina.
Click below to interact with the system
Examine how the following factors might impact Betty's predicted risk score, based on the Neural Network model utilized:
Note: This is a demo only. A full decision-support system will include other patient characteristics. 2 randomly chosen characteristics that impact the risk score were included here. This interactive tool is not meant to propose medical actions. Its goal is to enable exploring of how different patient characteristics may impact their risk score.
Predicted Risk Score:
83.5%
77.2%
77.6%
68.4%
61.7%
62.3%
Click below to view the details of a linear approximation model for Betty's Risk Strata of 80-100%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear regression models.
A different model is trained for each risk quintile, 0-20%, 20-40%, etc.
Below are the coefficients for all significant characteristics of Betty's local linear approximation model. Note that the magnitude of the coefficients signifies how much the patient characteristic contributes to the risk score.
Click below to view the details of a decision tree approximation model for Betty's Risk Strata of 80-100%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear decision tree models.
A different tree is trained for each risk quintile, 0-20%, 20-40%, etc.
Below is a representation of Betty's local depth-3 decision tree approximation.
Click below to find the patient's status 1 year after the heart failure event
Patient Betty unfortunately passed away 3 months following her heart failure event.
Based on the information seen so far, including Patient Betty, how satisfied would you expect an average doctor to be with the Decision Support System powered by a Neural Network model?
1: Completely unsatisfied, not at all likely to use the system in supporting their medical decision-making for heart failure patients
2: Fairly unsatisfied, not likely to use the system
3: Neither satisfied nor unsatisfied, may or may not consult system
4: Somewhat satisfied, likely to at least take a look at the system's predicted risk score
5: Highly satisfied, very likely to consult the system and its prediction as part of their medical decision-making for heart failure patients
Please provide any comments or reasons supporting your answer:
The following represents a patient scenario. A Decision Support System outputs a risk score based on the patient's characteristics. A doctor may choose to use the information below, including the risk score, to inform their medical decisions.
Our model predicts that the probability of Clara dying in the one year following the event is 60.5%.
Clara has a BMI of 33.4, and exhibits rales and shortness of breath at rest.
Clara has some limitation of physical activity (New York Heart Association Score Class II).
Clara has been prescribed ACE inhibitors.
Clara is diabetic, and smokes regularly.
Click below to interact with the system
Examine how the following factors might impact Clara's predicted risk score, based on the Neural Network model utilized:
Note: This is a demo only. A full decision-support system will include other patient characteristics. 2 randomly chosen characteristics that impact the risk score were included here. This interactive tool is not meant to propose medical actions. Its goal is to enable exploring of how different patient characteristics may impact their risk score.
Predicted Risk Score:
60.5%
61.0%
61.3%
54.2%
54.6%
54.9%
Click below to view the details of a linear approximation model for Clara's Risk Strata of 60-80%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear regression models.
A different model is trained for each risk quintile, 0-20%, 20-40%, etc.
Below are the coefficients for all significant characteristics of Clara's local linear approximation model. Note that the magnitude of the coefficients signifies how much the patient characteristic contributes to the risk score.
Click below to view the details of a decision tree approximation model for Clara's Risk Strata of 60-80%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear decision tree models.
A different tree is trained for each risk quintile, 0-20%, 20-40%, etc.
Below is a representation of Clara's local depth-3 decision tree approximation.
Click below to find the patient's status 1 year after the heart failure event
Patient Clara was alive one year after her heart failure event. However, she passed away 2 years later.
Based on the information seen so far, including Patient Clara, how satisfied would you expect an average doctor to be with the Decision Support System powered by a Neural Network model?
1: Completely unsatisfied, not at all likely to use the system in supporting their medical decision-making for heart failure patients
2: Fairly unsatisfied, not likely to use the system
3: Neither satisfied nor unsatisfied, may or may not consult system
4: Somewhat satisfied, likely to at least take a look at the system's predicted risk score
5: Highly satisfied, very likely to consult the system and its prediction as part of their medical decision-making for heart failure patients
Please provide any comments or reasons supporting your answer:
The following represents a patient scenario. A Decision Support System outputs a risk score based on the patient's characteristics. A doctor may choose to use the information below, including the risk score, to inform their medical decisions.
Please examine the following patient:
Patient Drew, a 70-year-old non-Caucasian male, experienced heart failure.
Our model predicts that the probability of Drew dying in the one year following the event is 72.0%.
Drew has a BMI of 24.2, and exhibits rales and shortness of breath at rest.
Drew is unable to perform physical activity without discomfort (New York Heart Association Score Class IV).
Drew has been Not been prescribed ACE inhibitors or Beta blockers.
Drew is diabetic, but Drew does does not effectively manage his diabetes. He is a non-smoker.
Click below to interact with the system
Examine how the following factors might impact Drew's predicted risk score, based on the Neural Network model utilized:
Note: This is a demo only. A full decision-support system will include other patient characteristics. 2 randomly chosen characteristics that impact the risk score were included here. This interactive tool is not meant to propose medical actions. Its goal is to enable exploring of how different patient characteristics may impact their risk score.
Predicted Risk Score:
72.0%
77.8%
64.4%
73.9%
Click below to view the details of a linear approximation model for Drew's Risk Strata of 60-80%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear regression models.
A different model is trained for each risk quintile, 0-20%, 20-40%, etc.
Below are the coefficients for all significant characteristics of Drew's local linear approximation model. Note that the magnitude of the coefficients signifies how much the patient characteristic contributes to the risk score.
Click below to view the details of a decision tree approximation model for Drew's Risk Strata of 60-80%
Machine Learning models, including the neural network powering this decision-support system, can be approximated locally using simpler, highly interpretable linear decision tree models.
A different tree is trained for each risk quintile, 0-20%, 20-40%, etc.
Below is a representation of Drew's local depth-3 decision tree approximation.
Click below to find the patient's status 1 year after the heart failure event
One year after his heart failure event, Patient Drew was alive. He unfortunately passed away 16 months following his heart failure event.
Based on the information seen so far, including Patient Drew, how satisfied would you expect an average doctor to be with the Decision Support System powered by a Neural Network model?
1: Completely unsatisfied, not at all likely to use the system in supporting their medical decision-making for heart failure patients
2: Fairly unsatisfied, not likely to use the system
3: Neither satisfied nor unsatisfied, may or may not consult system
4: Somewhat satisfied, likely to at least take a look at the system's predicted risk score
5: Highly satisfied, very likely to consult the system and its prediction as part of their medical decision-making for heart failure patients
Please provide any comments or reasons supporting your answer:
Part 3: Reflection
Based on both the Model Information seen in Part 1 and the patient scenarios seen in Part 2, please answer the following:
Do you feel that the neural network model presented, which was used to power a decision-support system, can augment the judgement of medical experts and constitutes a valuable contribution to medical decision-making processes?
Yes
No
Please explain why or why not:
Part 4: Comments
Please leave any feedback, comments, or concerns about the survey you have just completed.
In particular, you may address the following:
What are your general thoughts of Machine Learning in decision-support systems for prognostic predictive purposes?
Did you find any of the model evidence and other information shown in Part 1 particularly effective or ineffective? Why?
Do you view the patient scenarios shown in Part 2 as helpful in developing doctors' confidence in the underlying model and system? Why or why not?
Were there any areas of the survey you felt were confusing or potentially misleading?
Important: Do not include any personally identifiable information, such as name or email address, in your answer below.
You may also email the primary researcher at oren.lahav@gtc.ox.ac.uk.
Finished!!!
Thank you very much for taking our survey. Your anonymous results will be used as part of a statistical and ML analysis to determine the best evidence to present to potential users of decision-support systems that rely on sophisticated ML models.
We trust that your efforts will be highly significant in helping design Decision-Support systems for prognostic predictions based on Machine Learning models that are useful and make valuable contributions to prognostics and medicine in general.
Thank you!




Part 4: Comments
Please leave any feedback, comments, or concerns about the survey you have just completed.
In particular, you may address the following:
Important: Do not include any personally identifiable information, such as name or email address, in your answer below.
You may also email the primary researcher at oren.lahav@gtc.ox.ac.uk.